+90-548-875-8000
+90-548-876-8000
Elite Hospital
North Cyprus
Follow Us on
Social Media
Any patient who has been through an IVF cycle or is planning to undergo one has come across with certain IVF jargon. There are different names for different IVF protocols and there are different types of medication used in these protocols.
Furthermore, different IVF specialists may prefer different brands of IVF medication and some use additional supplements which are not used by others!
This all becomes very confusing especially when there is so much relevant and irrelevant information on the internet and one can’t help but wonder if she is using the right protocol or the medication in her IVF cycle.
On this page, we aim to mention brief differences between different IVF protocols and outline main characteristics of IVF medication and explain how they work. As North Cyprus IVF Center, we prefer some brands over others when prescribing medication and on this page we explain our reasons behind our medication choices.
There is one purpose of an ovulation induction protocol: To obtain an optimal number and quality of eggs (oocytes) so that success with the IVF cycle can be maximized. While the more is not necessarily the merrier when it comes to egg count, an IVF specialist will want to find the right balance between the number and quality of eggs to be obtained. Many patients think that the higher the number of eggs, the higher the chances of IVF success but this is not necessarily the case. Too many eggs can possibly lead to hyper-stimulation of the ovaries, which, in turn, can potentially reduce the quality of your eggs. Therefore, there is a fine line between quantity and quality of eggs and that is why there are so many IVF protocols out there trying to get you that perfect balance.
One of the main factors considered when preparing a patient’s treatment protocol is the age of the patient. Besides age, hormone levels and ovarian function are considered when deciding whether down regulation is needed or how much of it is needed. Based on the patient’s age, her hormone levels, her ovarian function and menstrual period information, there are two main categories of IVF protocols which may be selected. These are:
An agonist protocol is the one where the patient’s hormone release is down-regulated using an agonist such as Leuprolide acetate in the form of injections or nasal spray. The purpose of a Gonadotropin-releasing hormone agonist (GNRH-a) is to temporarily silence the pituitary release of the patient’s own hormones, which is also known as down-regulation. Temporarily silencing the patient’s own gonadotropins allows the IVF specialist to have a greater control over the IVF cycle for better manipulation of the ovaries via ovulation induction. Administration of an agonist suppresses the pituitary response and inhibits secretion and release of gonadotropin hormones (FSH and LH) and puts the ovaries in a temporary state of “hypogonadotropic hypogonadism”.
There exist three types of agonist protocols:
While long protocol is preferred for patients with sufficient ovarian function and regular menstrual periods, the microdose flare protocol is preferred for the poor-responder group. If the patient has lower ovarian function, placing her on the standard long protocol can cause too much suppression of the ovaries and the patient may nor respond well to the ovulation induction protocol to be followed later on as her ovaries will not be able to recover from the state of hypogonadism in a short period of time. For poor responders, the microdose (low dose) flare protocol is preferred where the lenght of treatment is identical to the long down-regulation protocol but the dose of down-regulation is much smaller.
The short protocol is no longer preferred as research and clinical studies have shown no real benefits of using the short protocol over other two types of agonist protocols or the antagonist protocol.
An antagonist protocol does not suppress or down-regulate the ovaries prior to starting with controlled ovarian hyperstimulation (ovulation induction). Research and clinical studies have shown evidence that using an antagonist protocol can provide more favorable results for patients in the poor-responder group. Antagonist protocol is also likely to generate a higher number of follicle growth with smaller doses of gonadotropins during an IVF treatment for this patient group. We also prefer to use this protocol for patients with poly cystic ovaries / poly cystic ovarian syndrome (PCO/PCOS) as it gives a much higher control over managament of hyperstimulation compared to the agonist protocols.
At North Cyprus IVF Center, we recommend our patients to start using a prenatal vitamin complex prior to embryo transfer. Prenatal vitamins help obtain the vitamins and minerals necessary during pregnancy in the right amounts. Starting a bit earlier than embryo transfer will help your body to adjust its physiology accordingly.
Patients who are in the “poor responder” group, and patients whose oocytes have been found to be of sub-optimal quality after an IVF cycle are recommended to use inofolic Sachets for 8 weeks until the day of egg retrieval. Even though this was originally designed for patients with PCOS, many studies have found that using 4 grams of inofolic sachets a day (inositol + folic acid) helps with oocyte quality in poor responder women.
Patients in older age brackets who still have an acceptable level of ovarian function can be suitable for use of human growth hormone prior to their IVF treatment. Human growth hormone, when used for a certain period of time before ovulation induction can help correct some of the genetic defects associated with oocyte aging. Therefore, patients over the age of 40 with an acceptablle level of ovarian reserves are suitable candidates for this program.
Medication used during the IVF cycle aim to recruit follicles for ovulation, help with maturation and prepare the endometrium for a successful embryo implantation. At North Cyprus IVF Center, below are the main categories of medication used for ovulation induction and endometrial preparation:
Femara 2.5 mg (Letrezole) tablets during the first few days of menstrual cycle can be used for patients in the poor-responder group. Femara is a drug which belongs in the “aromatase inhibitors” classification of drugs. As suggested by its name, femara inhibits the enzyme aromatase. When this enzyme is inhibited, it silences the estrogen receptors, therefore, estrogen levels are suppressed. The reason why we would like to suppress the estrogen levels during the first few days of the menstrual cycle is because during this stage, the developing follicles release estrogen, and with the release of estrogen, the negative feedback mechanism between the ovaries and the hypothalamus is activated so the FSH release can be reduced. We do not want FSH to reduce because FSH helps us recruit more follicles for ovulation since follicles are very FSH dependent during the first few days of the menstrual cycle.
Gonal F as opposed to Menopur: The first 4 days of the menstrual period (the follicular phase) is when the follicles are FSH dependent and they have no use for LH (because LH is involved in oocyte maturation, not recruitment). Gonal-F is a pure FSH supplementation. However, Menopur is an FSH+LH supplement. Therefore, Menopur contains a certain amount of LH which is simply unnecessary. It may not harm you, but it also doesn’t do any good and takes away from the dosage of medication that you are supposed to take. Therefore, Gonal-F should be preferred for the first 4 days of your ovulation induction and then we can use a combination of Gonal-F and Menopur.
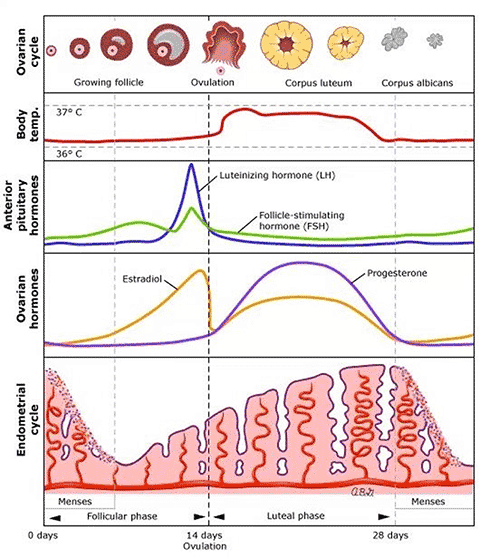
Figure to the right (bottom on mobile) shows what happens during an ovarian cycle in a given month. In this figure, we can see the levels of various hormones during a menstrual cycle. The green line shows FSH levels while the blue line shows LH levels during a natural cycle. Given that what we try to do during an IVF cycle is to mimic the nature, it is our aim to maintain a similar ratio.
As can be seen on the diagram, FSH levels are much higher compared to LH levels prior to ovulation. LH, in fact, rests at a baseline level with no increase in value up until the LH surge which takes place prior to ovulation. The reason for this is, primary follicles (small follicles before they turn into antral follicles) develop receptors to follicle stimulating hormone (FSH), but they are gonadotropin-independent until the antral stage. Once they reach the antral follicle stage, the FSH receptors become sensitized and the presence of FSH helps them develop. However, an increased level of LH is not required because the follicles are not yet ready to mature at this point.
Progesterone supplements are used immediately after egg collection. In a natural menstrual cycle, progesterone production starts immediately after ovulation. This is not a coincidence. If you look at the top of the diagram, you will see that once the follicle reaches ovulation, the egg is released and the remaining parts of the follicle become what’s known as the “corpus luteum”. If ovulation results in a pregnancy, the corpus luteum becomes responsible for progesterone release and this helps maintain a healthy pregnancy.
During an IVF cycle, all your follicles are collected during an “oocyte pick-up / OPU” procedure. When your follicles are collected, they are denuded to obtain oocytes and the rest of the follicles are thrown away. This means you will not have a corpus luteum to help with progesterone release. Therefore, we prescribe you with external progesterone supplements so that the progesterone levels can be kept at what they should be during pregnancy until the placenta forms and takes over progesterone production. This happens around week 11 of pregnancy, and that is when we stop supplementing you with external progesterone.